Contact Us

January 10, 2019
Overview of Sigmoid Colon Vaginoplasty for MtF (Sigmoid Colon SRS)
MtF Vaginoplasty is a male to female Gender Reassignment Surgery procedure that transforms natal male genitals into a functional, aesthetically pleasing vagina. With a qualified surgeon, patients can expect normal urination, sexual sensation, and minimal scarring.
The ultimate goal of MtF Vaginoplasty is a vagina that is secretory, flexible, hairless and pink, and approximately 5-7 inches in depth and about 1-1.5 inches in diameter. There are multiple MtF Vaginoplasty techniques used around the world to achieve this goal, but the two most common are Penile Inversion Vaginoplasty and Rectosigmoid Vaginoplasty. The skin graft is normally used for the vaginal lining during sex reassignment surgery (SRS), however the colon graft can also be used as an alternative surgical procedure in primary sex change surgery as well as corrective surgical procedure in the post-status SRS patients who have unsatisfactory depth of vagina.
Understanding the basics of each technique will help you make a more informed decision about which one is right for you. Today, in this article, we are going to discuss everything that you need to know about the Rectosigmoid Vaginoplasty before you make a decision.
Sigmoid Colon Vaginoplasty
Rectosigmoid Vaginoplasty, aka Sigmoid Colon Vaginoplasty, uses a section of the sigmoid colon to create the vaginal lining. It is an intrusive procedure in which the intra-abdominal cavity must be entered via a low transverse abdominal incision (like Caesarean section incision in biological female). However, Rectosigmoid Vaginoplasty results in a well-proportioned, self-lubricating vagina, which has less risk of losing vaginal depth. Furthermore, this segment of the colon is thick-walled and large in diameter and flexible. The technique is particularly suited to patients who have short penis or have orchiectomy done previously, and is also used as a corrective surgery for patients with vaginal obstruction as the result of a previous SRS.
A sigmoid colon section approximately 6-7 inches in length is harvested as a pedicle flap, with the neurovascular bundle, through an abdominal incision, then the rest of the colon is reconnected. The sigmoid colon section is connected to the perineum using genital skin flaps. orchiectomy, penectomy, labiaplasty and clitoroplasty are also performed as required. The surgery lasts approximately 6-7 hours.
Criteria for Sigmoid Colon Vaginoplasty
▪ Patient’s BMI (Body Mass Index) must be less than 25.
▪ Patient must not have any bowel disease or undergo any bowel surgery before.
Pre-operative preparation
▪ Need to prepare the bowel cleansing one night before the surgery by enema and laxative
▪ Liquid diet 3 days before the surgery
▪ Antibiotics 48 hours before the surgery
▪ Discontinue hormones (including spironolactone) prior to the surgery, 2 weeks for oral tablets and 4 weeks for injection.
▪ Stop smoking 2 weeks prior to the surgery
▪ Discontinue drugs that may interfere with blood clotting, such as aspirin, ibuprofen andvitamin E
Post-operative care
▪ Wound cleansing
▪ Dilation
▪ Low residue diet for 1-2 months
Disadvantages of Sigmoid Colon SRS
▪ Additional abdominal surgery with intestinal anastomosis, which increases the risk ofpostoperative ileus.
▪ Visible small abdominal scar.
▪ A longer surgery with added complexity and expense.
▪ The production of mucus from the colon graft can lead to excessive discharge although thistypically decreases significantly within 3–6 months. (Daily vaginal cleaning for 1 month can help.)
▪ Colon grafts must be screened for colon cancer and should be monitored if the patient develops inflammatory bowel disease.
Disadvantages of Sigmoid Colon SRS
▪ Additional abdominal surgery with intestinal anastomosis, which increases the risk ofpostoperative ileus.
▪ Visible small abdominal scar.
▪ A longer surgery with added complexity and expense.
▪ The production of mucus from the colon graft can lead to excessive discharge although thistypically decreases significantly within 3–6 months. (Daily vaginal cleaning for 1 month can help.)
▪ Colon grafts must be screened for colon cancer and should be monitored if the patient develops inflammatory bowel disease.
Possible long-term complication
▪ Intestinal obstruction (Adhesion band)
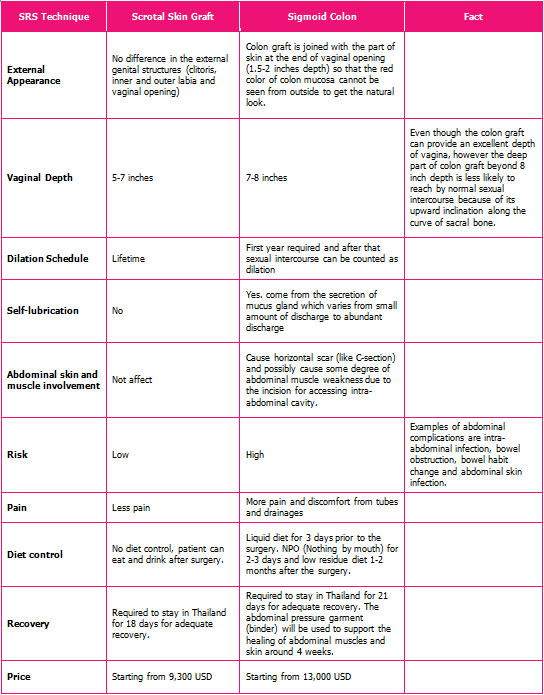
Comparison of Standard SRS (Skin Graft technique) and Sigmoid Colon SRS (Colon Graft technique)
How to Choose?
The choice of which MtF Vaginoplasty technique to pursue is dependent upon a number of factors, including your surgeon's experience with a particular technique, your anatomy, and most importantly, your goals. Consider the advantages and disadvantages of the techniques, as well as what's most important to you with your surgery outcome, and bring your questions and concerns to your surgery consult. Together, you and your surgeon can make the final decision about the right MtF Vaginoplasty technique for you.
Source:
http://www.chet-plasticsurgery.com/colon-graft-technique/
https://www.mtfsurgery.net/mtf-vaginoplasty.htm
extra08-09-transgendersurgerythailand_com
Gender reassignment surgery - Contact us
Messages : estetica.thailandia
Email : [email protected]
Other Blog Page
-
Understanding the Importance of Pre-operative Genital Hair Removal for MtF Gender Reassignment Surgery
-
SRS IN THAILAND DURING COVID-19 : PROCESS OF ENTRY
-
Introducing “Diamond technique”
-
Your SRS Trip to Thailand: Getting Ready for it!
-
Facial Feminization Surgery (FFS) in Thailand with Estetica Thailandia
-
What You Need to Know Before Deciding to Do Cosmetic Surgery in Thailand
-
Which SRS technique is right for me?
-
How to Start Your SRS Trip with Us
-
Research Overview on the Life-Changing SRS Journey to Find Your True Self and Happiness
-
Is Labiaplasty Needed After Sex Reassignment Surgery (SRS)?
-
How To Reduce Pain After Facial Feminization Surgery (FFS)
-
Overview of Sigmoid Colon Vaginoplasty for MtF (Sigmoid Colon SRS)
-
7 Reasons Why You Need Our Service
-
Frequently Asked Questions about Sex Reassignment Surgery (SRS)
-
Advance Sex Reassignment Surgery Techniques
-
Tracheal Shave in Facial Feminization Surgery
-
What I Wish I’d Known Before Undergoing Sex Reassignment Surgery
-
Post-Operative Care Is Vital to Your SRS Journey
-
5 Things you Need to Know Before Sex Reassignment Surgery in Bangkok
Where your dream come true
What we do
Gender Reassignment Surgery (GRS)
Penile Skin Inversion with scrotal skin graft
Breast augmentation
Labiaplasty (post-op revision)
Penile Skin Inversion with abdominal skin graft
Facial Feminization Surgery(FFS)
